
Understanding and Managing Postoperative Nausea and Vomiting (PONV)
What is Postoperative Nausea and Vomiting (PONV)?
PONV refers to the nausea and vomiting that some patients experience after undergoing surgery. It can occur within the first 24 hours post-surgery and significantly impacts patient comfort and recovery. Understanding the mechanisms and risk factors associated with PONV is crucial for implementing effective prevention and treatment strategies.
Causes of PONV
The exact cause of PONV is multifactorial and not entirely understood, but it involves a combination of patient-specific, surgical, and anaesthetic factors. Key mechanisms include:
-
Stimulation of the Vomiting Centre: Surgical procedures, especially those involving the gastrointestinal tract, middle ear, or brain, can stimulate the brain's vomiting centre.
-
Anaesthetic Agents: Volatile anaesthetics, nitrous oxide, and opioid analgesics are known to trigger nausea and vomiting.
-
Gastrointestinal Factors: Delayed gastric emptying and swallowed blood during surgery can contribute to nausea.
Risk Factors for PONV
Understanding the risk factors helps in identifying patients at higher risk and implementing preventive measures. Risk factors include:
-
Patient Factors:
-
Female gender
-
Non-smoker status
-
History of motion sickness or previous PONV
-
Younger age
-
Surgical Factors:
-
Type of surgery (e.g., laparoscopic, gynaecological, or ENT surgeries)
-
Duration of surgery
-
Anaesthetic Factors:
-
Use of volatile anaesthetics
-
Use of nitrous oxide
-
Use of postoperative opioids
Preventive Strategies
Prevention is key in managing PONV. Strategies include:
-
Risk Assessment: Utilise risk scores, such as the Apfel score, to identify high-risk patients.
-
Pharmacologic Prophylaxis: Administer antiemetics prophylactically. Common agents include:
-
Serotonin (5-HT3) antagonists: Ondansetron
-
Dopamine antagonists: Droperidol, Metoclopramide
-
NK-1 receptor antagonists: Aprepitant
-
Steroids: Dexamethasone
-
Antihistamines: Dimenhydrinate
-
Multimodal Approach: Combining different classes of antiemetics can be more effective than using a single agent.
-
Non-Pharmacologic Measures: Techniques such as acupuncture, acupressure, and adequate hydration can complement pharmacologic methods.
Management of Established PONV
Despite preventive measures, some patients will still experience PONV. Effective management includes:
-
Reassessment: Determine the severity and possible causes of PONV.
-
Pharmacologic Treatment: Administer antiemetics not used in the prophylactic regimen to avoid tachyphylaxis.
-
Hydration and Electrolyte Balance: Ensure adequate hydration and correct any electrolyte imbalances, which can exacerbate nausea and vomiting.
-
Patient Comfort: Provide a calm environment and reassure the patient to help reduce anxiety-related nausea.
Click the image above to expand.
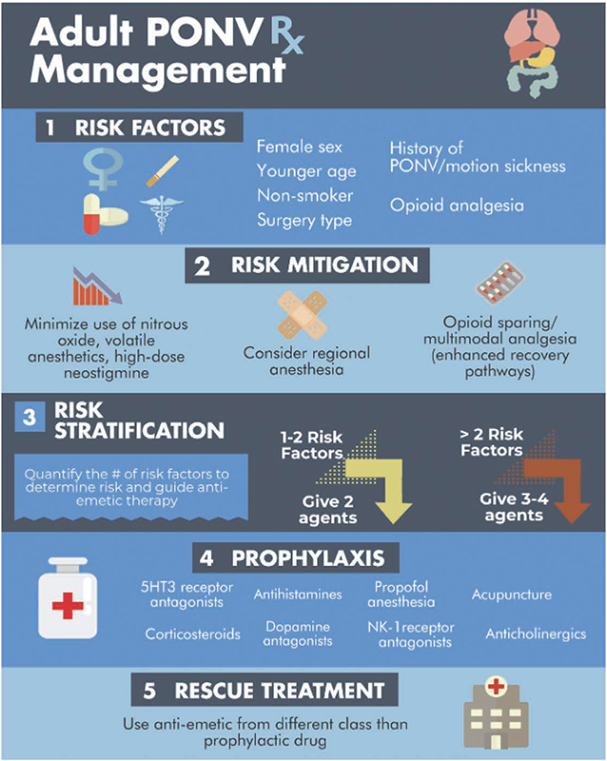
Algorithm for PONV management in adults. Summary of recommendations for PONV management in adults (Gan et al 2020)
PONV is a challenging but manageable aspect of postoperative care. By understanding the underlying mechanisms, identifying at-risk patients, and implementing effective preventive and treatment strategies, perioperative professionals can significantly improve patient outcomes and comfort. Continuing education and staying updated with the latest guidelines and research are essential for optimising the management of PONV in the perioperative setting.
Related courses
- Post-operative Clinical Deterioration
- Perioperative therapeutics, from anaesthesia to analgesia: Perioperative Nursing Update Module 3
- Lunch and Learn: Post Operative Nausea & Vomiting
References

DebEvans, RN, BSc, DipAnaes&PostAnaesNsg, CritCareCert, DipProfStudies, Teach&AssessClin.PractCert, CertIV(TAE) has extensive background in Perioperative education and management. Deb has worked overseas and in several tertiary hospitals in Brisbane as an educator and manager including the Mater & The Wesley Hospital where she was awarded CEO Award for Innovation and Excellence and The Spirit of Wesley Staff Award for commitment to Quality and Safety.
Deb has developed blended education programs within the perioperative environment to include; Graduate transition programs; Clinical mandatory training; Corporate required learning & Point of Care SIMs; Perioperative competency development skills and speciality training programs. She recently worked for Montserrat Day Hospitals as the National Education & Training Manager and implemented a virtual orientation program, LMS & introduced speciality learning pathways. Deb has also been an ALS instructor & involved with a range of universities as a clinical facilitator and a lecturer at TAFE.
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreMedcast Education
Sepsis is a time-critical medical emergency. The National Sepsis Program urges GPs and primary care clinicians to enhance early recognition and management of sepsis to save lives. This update outlines key actions and available resources to support timely diagnosis and intervention across primary care settings.
James, a university student with a history of seasonal allergic rhinitis, presents with sudden respiratory distress following exposure to grass pollen during a soccer game shortly before a summer thunderstorm. Could this be thunderstorm asthma?
This article addresses challenges in managing the healthcare needs of Minh, who is a patient with an intellectual disability and complex communication needs. It emphasises the importance of understanding individual communication methods, obtaining proper consent, and collaborating with support teams.