
Massive Transfusion Protocol - Understanding the clotting cascade
The Clotting Cascade: A Vital Process in Bleeding Management
When faced with a bleeding patient, understanding the intricacies of the clotting cascade, and the pivotal role these processes have in managing bleeding provides the foundation for integration of therapeutic guidelines into clinical practice. This cascade involves a sequence of events that kick into action whenever there's damage to the blood vessels. Whether it's a surgical procedure or trauma, the body's response involves processes designed to restore haemostasis and prevent excessive bleeding.
Activation of the Clotting Cascade
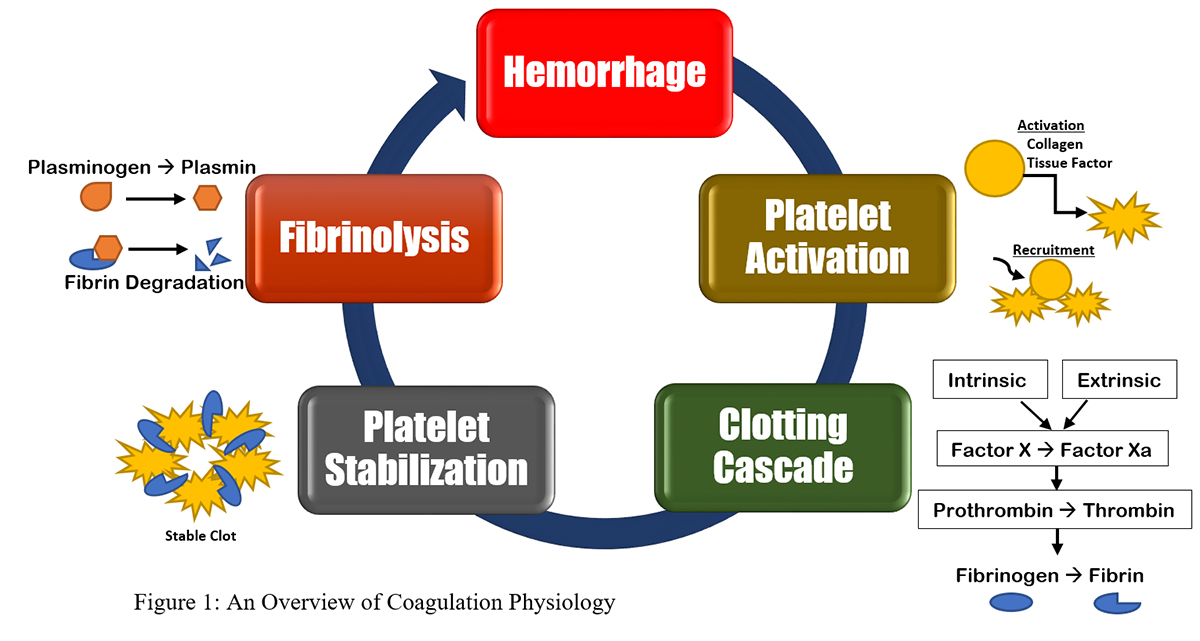
Image source: McLaughlin C. (2023)The physiology of coagulation and blood product transfusions JEMS
The clotting cascade is an efficient process between various factors and components. When the endothelium, the lining of blood vessels, experiences damage, both the intrinsic and extrinsic pathways of the clotting cascade are activated. This marks the beginning of a sequence that ultimately leads to the formation of a stable clot.
Platelets and Factor X: Building Blocks of Clot Formation
As the cascade begins, platelets are released to the site of injury. These tiny blood cells play a pivotal role in forming the initial foundation of the clot. Factor X, a crucial player in the cascade, is activated and prompts the production of prothrombin. Prothrombin is then converted into thrombin, which acts as the catalyst for fibrinogen to transform into fibrin. This mesh of fibrin covers the platelet foundation, fortifying the clot and effectively controlling the bleeding.
However, it's important to note that this process isn't without consequences. The consumption of platelets and clotting factors is an inevitable part of this intricate sequence. As the clotting cascade progresses, these resources are utilised to ensure effective haemostasis.
Restoration of Haemostasis and Fibrinolysis
The clotting cascade's involvement doesn't end with the successful formation of a clot. The second part of the cascade is dedicated to restoring haemostasis and preventing an excessive or unnecessary buildup of clots. This is where fibrinolysis comes into play.
Activated plasminogen, a precursor, transforms into plasmin. The role of plasmin is to initiate the breakdown of the clot by dissolving the fibrin mesh, thereby ensuring that blood flow isn't obstructed once the damage is repaired and the clot is no longer needed.
The Finely Tuned Mechanism: Clot Formation and Dissolution
In essence, the clotting cascade is a finely tuned mechanism that combines both clot formation and dissolution to ensure efficient healing and prevent further complications. Understanding the balance between clot formation and fibrinolysis is crucial in managing bleeding disorders, postoperative care, and trauma cases.
Learn More - Clinical Application
Activation of the massive transfusion protocol is based on several clinical criteria. Most commonly the MTP or a Code Crimson is needed in trauma, obstetric and intra or postoperative emergencies. These protocols include specific strategies to manage the patient's clinical status, and maximise rational use of blood products.
Learn more in our:

Susan is the Head of Nursing Education for the Medcast Group.
DipAppScNsg, BN, CritCareCert, CoronaryCareCert, TraumaNsgCareCert, CertIV(TAE), MN(Ed), and GradCert(Ldrshp & Mgt).
Become a member and get unlimited access to 100s of hours of premium education.
Learn morePRECISE Education Team
Genetic testing in general practice: Dr. Alan Ma explains which tests GPs can order, when to refer, and how the PRECISE portal supports confident testing and referral decisions.
Dr Kate Annear
GP Dr Kate Annear and Clinical Psychologist A/Prof Aliza Werner-Seidler discuss practical strategies for engaging young people, conducting psychosocial assessments, and using lifestyle, social, psychological and digital interventions to support mild to moderate depression and anxiety in young people.
Medcast Medical Education Team
Many GPs may not see veterans frequently. This FastTrack provides a summary of key steps that can make veteran care efficient, rewarding and well-integrated into routine practice, including links to additional resources. 30mins each of RP and EA are available.