
Anthony is having frequent exacerbations of his COPD….why is his physician considering a GLP1 agonist?
Despite his health challenges, Anthony is compliant with his COPD and diabetes management. He regularly takes his medications as prescribed, attends follow-up appointments, and follows recommended lifestyle modifications. However, despite his efforts, he continues to experience exacerbations of his COPD.
Over the last couple of weeks Anthony tells you that he has been experiencing a notable increase in the frequency and severity of COPD exacerbations including worsening dyspnoea, cough and increased sputum. After performing spirometry tests, his results show a decrease in his FEV1 and FVC.
Is it time to add a GLP1 agonist to his treatment plan?
Given Anthony’s recent struggles with COPD exacerbations and the limitations of his current treatment regimen, exploring novel therapeutic options may be beneficial.
The potential benefits of introducing a GLP1 agonist will likely reduce the severity of his COPD symptoms due to the anti-inflammatory effects and potential reduction in airway hyperresponsiveness. There may be additional benefits in reduction of diaphragmatic pressure due to associated weight loss.
The biological mechanisms underlying these outcomes are as fascinating as they are promising. The reduction in local inflammation and airway hyperresponsiveness from GLP-1 receptor agonists, are crucial factors for managing COPD exacerbations. SGLT-2 inhibitors, on the other hand, may offer benefits by decreasing serum glucose concentrations, potentially reducing the burden on patients with difficulty expelling carbon dioxide.
GLP1 agonists, and SGLT2i are known for their favourable cardiovascular effects, there is now emerging evidence suggesting these drugs may also improve lung function for patients with COPD with improvement to FVC.
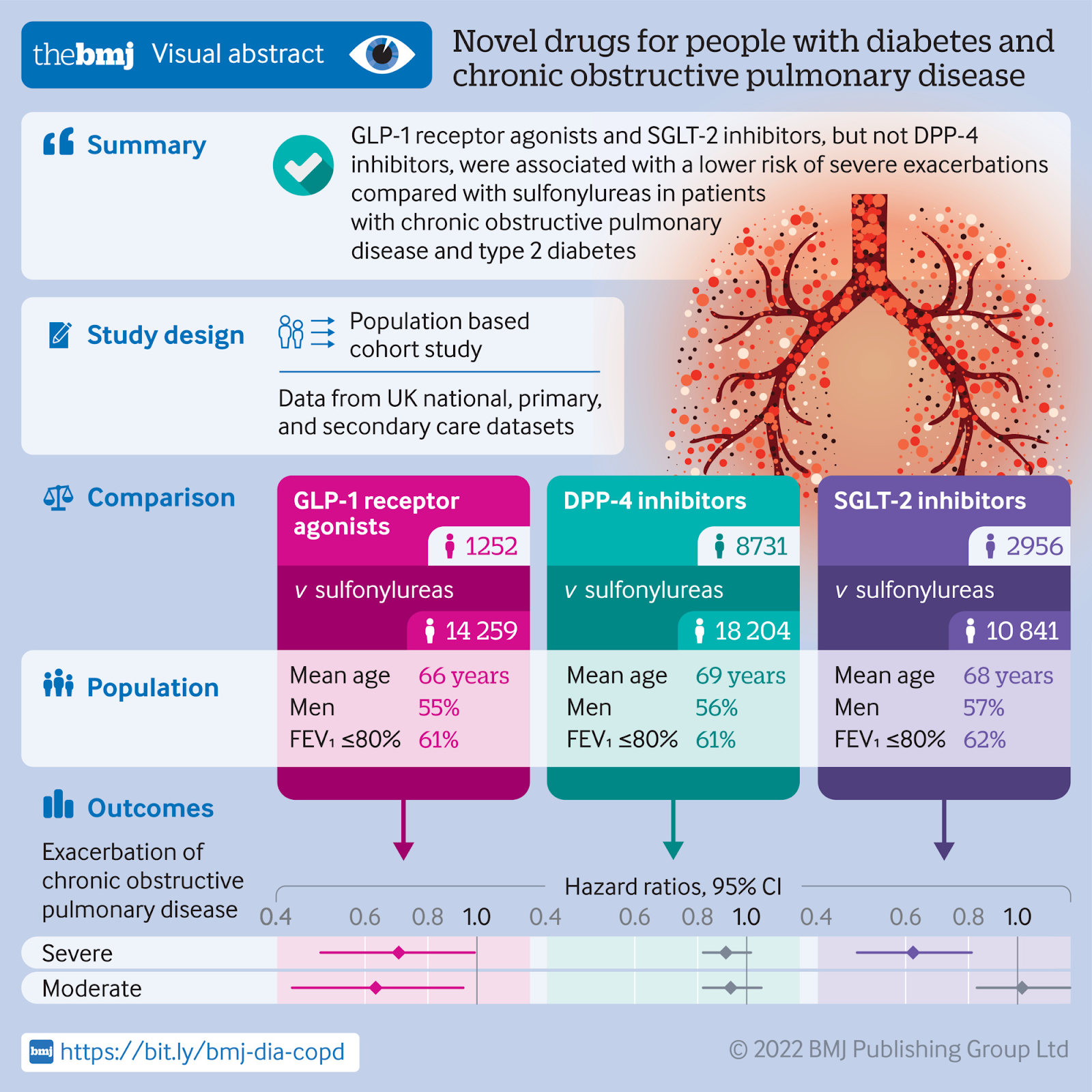
Reports from BMJ (Azoulay 2022) support a 30% reduction in severe exacerbation and 37% reduction in moderate exacerbations in COPD symptoms following the introduction of GLP1 agonists or SGLT2i compared to sulphonylureas. These results were an unexpected finding on the benefits of the novel anti-diabetic medications for managing chronic lung disease in patients with type 2 diabetes. The next question is whether this benefit extends to COPD patients without diabetes.
For GPs, these findings open up new therapeutic avenues for patients who present with this common comorbidity. The possibility of not just managing diabetes more effectively, but also mitigating the risk of COPD exacerbations, is an exciting prospect. It encourages a more integrated approach to patient care, considering the systemic interconnections between metabolic and respiratory health.
Related courses
References
-
Azoulay L (2022) Novel anti hyperglycemic drugs and prevention of chronic obstructive pulmonary disease exacerbations among patients with type 2 diabetes: population based cohort study BMJ 2022;379:e071380 https://doi.org/10.1136/bmj-2022-071380
-
Ng E., Shaw J., Wood A., Maple-Brown L., Hare M. (2022) Glucagon-like peptide-1 receptor agonist (GLP1-RA) therapy in type 2 diabetes AJGP Vol 51:7 doi: 10.31128/AJGP-07-21-6057 Glucagon-like peptide-1 receptor agonist (GLP1-RA) therapy in type 2 diabetes
-
GOLD Guidelines 2024 2024 GOLD Report - Global Initiative for Chronic Obstructive Lung Disease

Stephen is a GP Supervisor, Medical Educator, GP academic and Medical Director of Medcast. He has completed a PhD on Virtual Communities of Practice in GP Training.
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreMarjory is a 68 year old in-patient who is 2 days post hip replacement. She is on rivaroxaban (xarelto) for VTE prophylaxis. You find her sitting on the floor of the bathroom, alert but in pain.
We explore the case of Edward, a patient with acute kidney injury (AKI), focusing on renal protection strategies. It explores fluid management, blood pressure control, nephrotoxic drug adjustments, and electrolyte monitoring. Treatment considerations include vasoactive medications, dialysis options like CRRT, and medication dosing to support renal recovery and prevent complications.
James, a university student with a history of seasonal allergic rhinitis, presents with sudden respiratory distress following exposure to grass pollen during a soccer game shortly before a summer thunderstorm. Could this be thunderstorm asthma?