
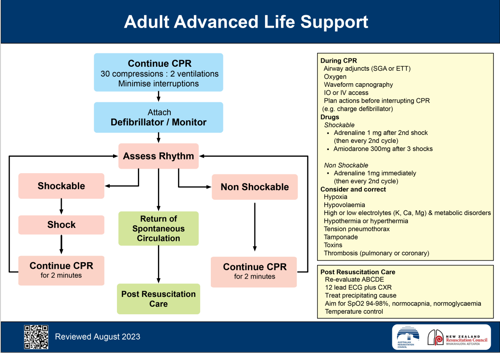
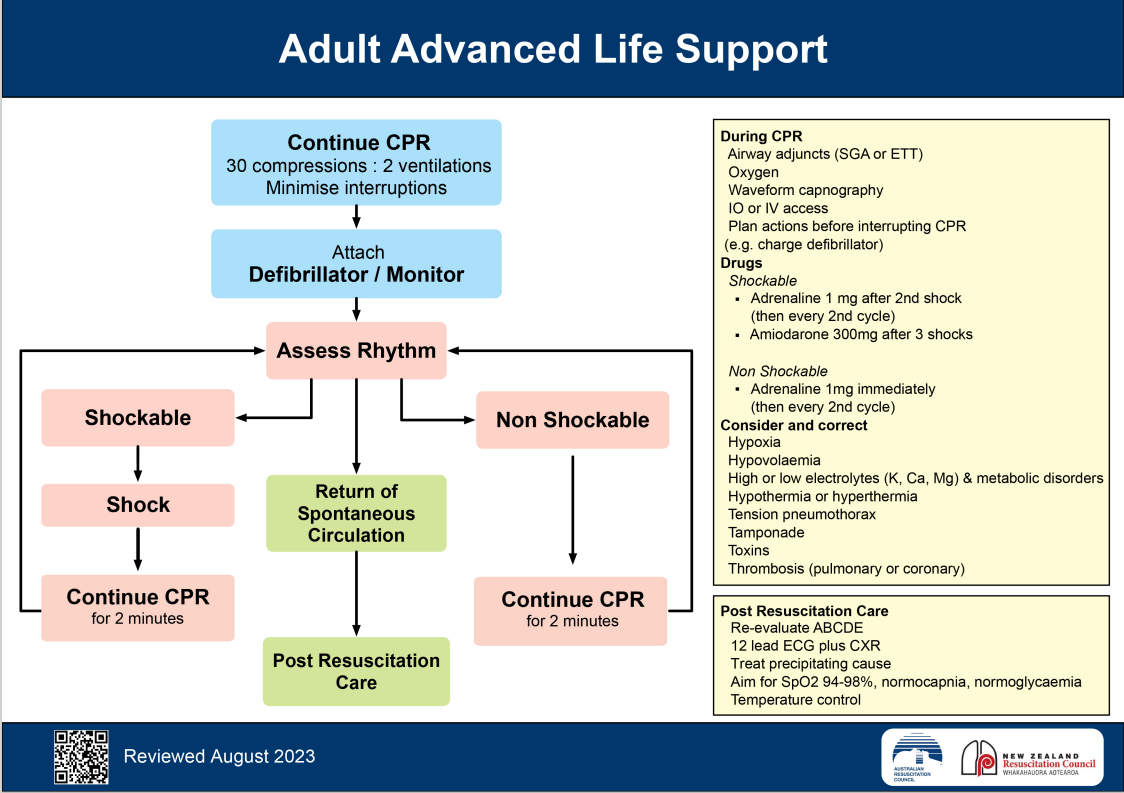
Revised ANZCOR Adult Advanced Life Support flowchart
Introduction to the ANZCOR 2023 Update
ANZCOR reviewed and up-dated the “Adult Advanced Life Support” flowchart in August 2023. This is the first revision since January 2016. The flowchart looks quite similar although there have been some wording changes.
The most significant changes are in the wording for the reversible causes and post-resuscitation care.
Click image to enlarge:
Key Changes in the Adult Advanced Life Support Flowchart
The flowchart on the left is basically unchanged except for the substitution of “ventilations” for “breaths”, and the addition of the word “continue” to CPR for 2 minutes on both the shockable and non-shockable sides of the flowchart following the rhythm check.
In the yellow boxes on the right of the flowchart, the prompt for airway adjuncts has replaced “LMA” with “SGA” to encompass both first and second generation supraglottic airways. The revised sentence “Plan actions before interrupting CPR (e.g. charge defibrillator)” is now more succinct. Rather than describing the 2 minutes of CPR as a “loop”, it is now referred to as a “cycle”
The reversible causes (the “4 Hs and Ts”) listed under “Consider and correct” are unchanged except now “Hyper/ hypokalaemia/ metabolic disorders” has been replaced with “High or low electrolytes (K, Ca, Mg) and metabolic disorders'' placing a greater emphasis on checking all of these electrolytes rather than potassium only. This will mean that ALS providers will need to be familiar with the treatments for high and low Calcium and Magnesium.
The Post Resuscitation Care section is unchanged except for the replacement of “Targeted temperature management” with “Temperature control”. Although ANZCOR guidelines continue to include targeted temperature management in their recommendations for patients who remain comatose at ROSC, these guidelines were based on limited trials in 2002, which indicated that temperature control targeted at 32–34 °C improved neurological outcome and mortality in patients who remained comatose after cardiac arrest.
More recent studies, however, have questioned the neuroprotective effects of hypothermia. The TTM-2 trial in 2021 showed no effect with temperature control targeted at 33 °C compared with normothermia or fever control. A systematic review of 32 trials published between 2001 and 2021 concluded that temperature control with a target of 32–34 °C compared with fever prevention did not improve survival or functional outcome following resuscitation.
Evidence-Based Insights on Temperature Control
Due to this growing body of evidence, the International Liaison Committee on Resuscitation (ILCOR) currently recommends monitoring core temperature and actively preventing fever (> 37.5 °C) for at least 72 hours in patients who are comatose after resuscitation from cardiac arrest. They no longer recommend therapeutic hypothermia for the treatment of patients who remain comatose at ROSC. As there was no difference found in the neurological outcome between patients treated with hypothermia and normothermia or fever prevention, ILCOR deemed that preventing fever had fewer side effects and required fewer resources than maintaining hypothermia.
Related Further Learning
References
-
ANZCOR Guideline 11.8 – Targeted Temperature Management (TTM) after Cardiac Arrest
-
ANZCOR Advanced Life Support for Adults Flowchart (2016)

Jenny Browne, RN, Cert IV (TAE), CritCareCert, MN(AdvClinEd), has an extensive background in critical care nursing and education. Jenny has worked across a variety of Australian ICUs, including the John Hunter Hospital (Newcastle), Princess Margaret Hospital (Perth) and the Royal Adelaide Hospital. She has been an ALS and PALS instructor for over 12 years, including with the ACCCN, and is also a sessional academic at the University of Newcastle.
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreA renewed partnership between Medcast and RACGP will ensure RACGP members have privileged access to discounted Basic Life Support training. The online course, meticulously aligned with guidelines, enables GPs to fulfil mandatory CPR course requirements.
This blog explores the ALS Algorithm and looks at how Medcast are trialling an adaptation of the 2023 updated ANZCOR Adult Advanced Life Support flowchart. The aim is to test its useability as a cognitive aid in ALS training to reduce cognitive load, enhance team performance and improve emergency decision-making.
Our courses have gained recognition for their comprehensive and practical approach to training healthcare professionals.