
Laryngospasm - Clinical Snapshot
Brett (15 years) was admitted for nasal polyp surgery. At the completion of the procedure a nasal endoscopy was performed and hyperplastic adenoids were found. The surgeons did not ressect the adenoids and did not communicate the findings.
The anaesthetist has just extubated Brett following waking him up and assessing his ability to obey commands. But he has just obstructed his airway, copious blood has been found and suctioned from his airway and a nasal airway is being placed.
You notice Brett’s Oxygen saturations dropping to 58%.
What is the next best step to take to improve Brett’s oxygenation?
Answer: Optimise airway opening manoeuvres
Failure to diagnose and successfully treat laryngospasm or any other form of airway obstruction may result in hypoxemia, bradycardia, negative-pressure pulmonary oedema, and cardiac arrest. Particularly in paediatric patients, laryngospasm is considered to be a significant factor in perioperative morbidity and mortality, cited as the proximate cause in 8% of paediatric cardiac arrests related to anaesthesia in a recent major review.
In the case of Brett 3 minutes of positive pressure CPAP was used to address the laryngospasm, but 1 hour later he became tachypneic oxygen saturations dropped to 85%. Following a chest x-ray indicating pulmonary edema affecting the left lung more than the right he was diagnosed with negative pressure pulmonary oedema.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7237060/
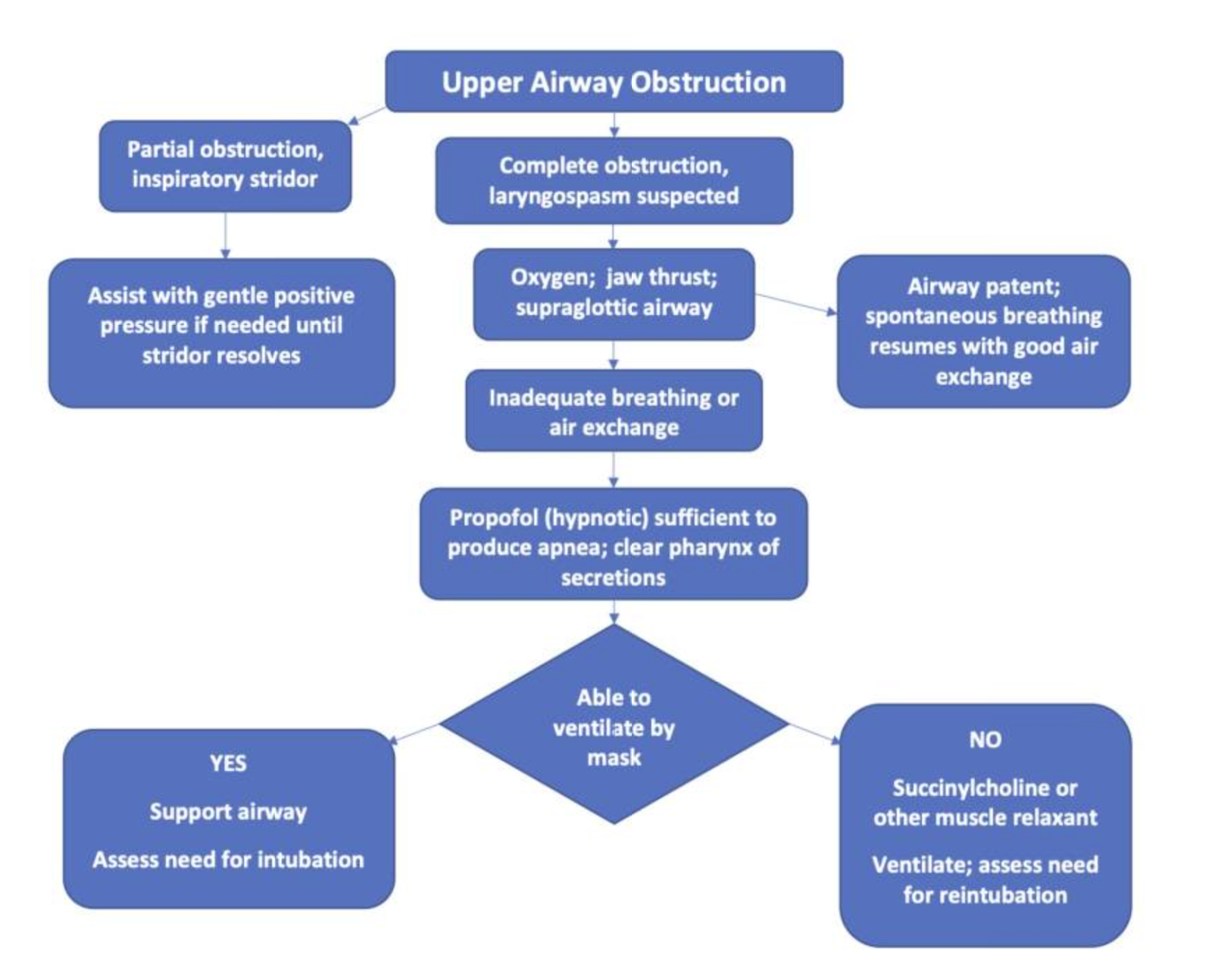
Treatment of laryngospasm
Treatment of laryngospasm should include:
-
Identification of laryngospasm
-
Sending for help
-
Removing stimulant if present with very careful suctioning of the airway(in this case blood)
-
Apply CPAP with 100 % oxygen, avoiding excessive pressure
If laryngospasm continues:
-
Deepen anaesthesia preferably with an I.V. bolus of propofol in 0.5 mg/kg increments and if that fails administering a muscle relaxant (I.V. succinylcholine is preferred)
-
If necessary, obtaining a definitive airway.
In this case study postoperative negative pressure pulmonary oedema was likely a result of the postoperative laryngospasm. Negative pressure pulmonary oedema is caused by strong respiratory efforts against a closed glottis or obstructed airway, which leads to strong hydrostatic pressures affecting the pulmonary vasculature, causing a transudative pulmonary oedema.
Full recovery and discharge
After 24 hours of treatment and observation Brett makes a full recovery and is discharged home.
Better communication regarding the adenoids from the surgical staff to the anaesthetist may have changed the extubation plan and subsequently reduced the risk of laryngospasm. Likewise administering a deeper anaesthetic or muscle relaxant earlier in the treatment pathway may have reduce the risk of the patient developing negative pressure pulmonary oedema.
This case reinforces the importance of interdisciplinary communication and of recognising and responding to laryngospasm.
Further learning and courses
- Can’t Intubate, Can’t Oxygenate CICO course
- Paediatric Advanced Life Support (PALS) course
- Perioperative Nursing Essentials course
References
https://www.aqihq.org/files/AIRS_8.18.pdf
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7237060/
https://www.bjanaesthesia.org.uk/article/S0007-0912(17)33310-X/fulltext

Grace Larson, RN, BN, CertIV(TAE), GradDipClinNurs(PaedCritCare), MAdNursPrac(PaedCritCare), has extensive experience in paediatric nursing, with 13 years in Paediatric Intensive Care Units (PICU). She’s published journal articles in the specialty area of pain and sedation in PICU, and has presented at national and international conferences on the area of pain and sedation in paediatrics. Grace has previously worked with the ACCCN delivering Paediatric Advanced Life Support in Victoria, bringing a wealth of experience into her clinical teaching on paediatric resuscitation. She has also consulted with NSW Health on quality and safety delivering within PICU, and has been contracted with the ANMF to develop nursing programs for nurses who require additional education as part of their practice requirements.
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreMarjory is a 68 year old in-patient who is 2 days post hip replacement. She is on rivaroxaban (xarelto) for VTE prophylaxis. You find her sitting on the floor of the bathroom, alert but in pain.
We explore the case of Edward, a patient with acute kidney injury (AKI), focusing on renal protection strategies. It explores fluid management, blood pressure control, nephrotoxic drug adjustments, and electrolyte monitoring. Treatment considerations include vasoactive medications, dialysis options like CRRT, and medication dosing to support renal recovery and prevent complications.
James, a university student with a history of seasonal allergic rhinitis, presents with sudden respiratory distress following exposure to grass pollen during a soccer game shortly before a summer thunderstorm. Could this be thunderstorm asthma?