
The protective role of pyrexia
Who hasn’t reached for the paracetamol when feeling under the weather with a cold or a patient presents with a fever? Are we doing the right thing, or does that fever have benefits in helping us fight the infection? Hippocrates claimed that
The HEAT trial (Young 2015) demonstrated that administration of paracetamol to patients with an infection/sepsis in the ICU did not reduce mortality. An elevated body temperature in response to infection sets in motion a series of mechanisms that regulate the immune system, these processes are important for fighting the infection, and administration of antipyretics such as paracetamol and ibuprofen will impede the body’s ability to perform this vital function.
In the presence of infective agents such as bacteria and viruses, pyrogens or fever producing proteins are released. These pyrogens act on the hypothalamus to release prostaglandin which resets the hypothalamic thermostat to a higher temperature resulting in an elevated body temperature.
In response to the release of pyrogens, the hypothalamus
- Conserves heat by triggering vasoconstriction (this has the added benefit of decreasing vascular pooling and optimising perfusion to organs) and
- Increases heat by triggering shivering
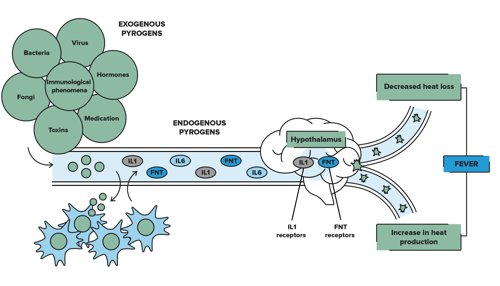
(Image adapted from Romera 2018)
How high is too high?
So why does paracetamol or ibuprofen routinely get prescribed and administered for fever? There is a downside to fever, for every 1℃ our body temperature increases there is a 10% increase in metabolism (Walter et al 2016). Our heart rate and respiratory rate increase and in some patients such as those with cardiac, respiratory or renal comorbidities this increased workload on the heart leads to complications.
This, and the fact that we ‘feel’ better, has led to the routine administration of antipyretics when fever is present.
Why you need to hesitate instead of administrate:
- The immune system works more efficiently when temperatures are elevated
- cytokine production is increased increasing the body’s ability to eliminate the pathogen
- Macrophages, neutrophils and T-cells respond faster and have an improved capacity to engulf and destroy pathogens at temperatures between 37.5 - 39.4℃
- Bacteria and viruses replicate easier at lower temperatures, an elevated body temperature will slow the multiplication rate reducing the severity of infection
(Walter et al 2016)
Next time you have a febrile patient, before you reach for the Paracetamol, ask yourself:
For further information consider the following courses
- PREPARED - Recognising and Responding to Clinical Deterioration
- Our PACED course explores childhood emergencies and outlines the physiological differences and pathways to deterioration in children
- Learn more about Sepsis in our Zero in on Sepsis webinar
- Maternal Sepsis - what you need to know
This article last reviewed by Susan Helmrich August 2023.
References and Further Reading:
Fajgenbaum D., & June C., 2020 Cytokine Storm N Engl J Med 383:2255-2273
Geddes L. (2020) The fever paradox New Science 246 (3277), 39-41
Liu Q., Zhou Y., and Yang Z. (2016) The cytokine storm of severe influenza and development of immunomodulatory therapy Cell Mol Immunol 13, 3-10
Romero M. (2018) How does fever occur? Clinic Barcelona Hospital Universitari
Walter E.J., Hanna-Jumma S., Carretto M., & Forni L. (2016) The pathophysiological basis and consequences of fever. Critical Care 20 (200)

Susan is the Head of Nursing Education for the Medcast Group.
DipAppScNsg, BN, CritCareCert, CoronaryCareCert, TraumaNsgCareCert, CertIV(TAE), MN(Ed), and GradCert(Ldrshp & Mgt).
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreFollow James, a 7-year-old boy scheduled for a tonsillectomy and adenoidectomy, as we explore how the 4 P’s of child preparation – Prepare, Play, Parent, Praise – can be used in day surgery to reduce procedural anxiety, support family-centred care, and improve the overall patient experience
Caregiver concern is a powerful predictor of clinical deterioration in children, often surpassing abnormal vital signs. A recent Lancet study confirms its association with ICU admission and ventilation. Integrating caregiver input into assessments, documentation, and escalation protocols can significantly improve early recognition and outcomes in paediatric emergency care.
Medcast Education
Sepsis is a time-critical medical emergency. The National Sepsis Program urges GPs and primary care clinicians to enhance early recognition and management of sepsis to save lives. This update outlines key actions and available resources to support timely diagnosis and intervention across primary care settings.