
Managing pacing failure in post-operative cardiac surgery: causes and solutions
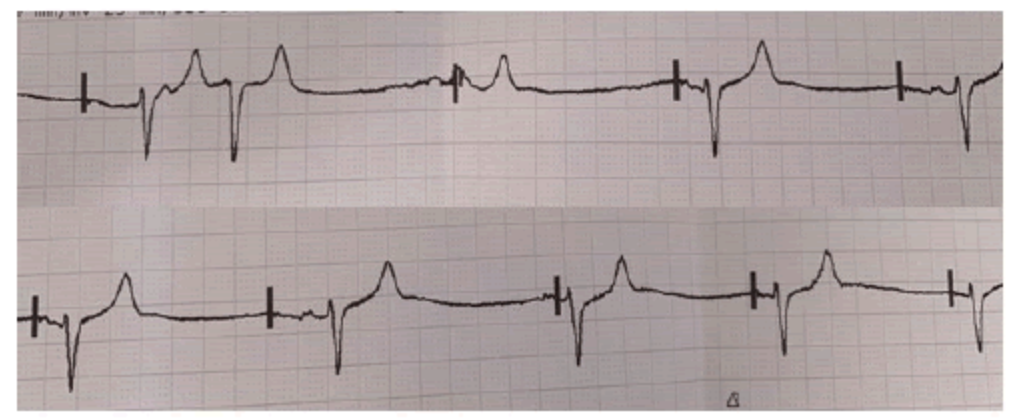
The emergency buzzer alarms in room 4, when you arrive you see Wayne pale and unconscious. The rhythm on the monitor displays the following:
Wayne is a 68-year-old male with a history of coronary artery disease, he underwent elective CABG surgery along with aortic valve replacement. His preoperative echocardiogram revealed preserved left ventricular function, but intraoperative findings showed extensive atherosclerosis, necessitating triple bypass.
On postoperative day 2, Wayne developed a third-degree atrioventricular (AV) block. This heart block manifested as dissociation between atrial and ventricular activity, with a ventricular rhythm of 30-35 beats per minute (bpm). Due to the critically low heart rate and resultant hypotension, the surgical team initiated temporary epicardial pacing using the leads placed during the operation.
He is being paced at DDD at a rate of 70 bpm on an output of 10mA.
His vital signs are as follows:
- Heart Rate: 32 bpm
- Blood Pressure: 82/56 mmHg
- SpO2: 94% on 4L/min oxygen via nasal cannula
- Respiratory Rate: 20 breaths per minute
- Temperature: 36.8°C
What is the issue with Wayne's pacemaker and what are 5 possible causes?
The issue: Failure to capture
Possible causes
Lead Malposition or Dislodgement
Temporary epicardial leads, which are placed on the heart’s surface during surgery, can become dislodged, leading to poor contact with the myocardium and failure to deliver the electrical impulse effectively.
Inadequate Pacing Output
While the initial pacing output was set at 10 mA, it may have been insufficient due to increased impedance in the leads or myocardial tissue changes post-surgery (e.g., edema or fibrosis).
Lead or Pacemaker Malfunction
Technical issues with the pacemaker generator or leads could prevent effective delivery of electrical stimuli. Faulty lead connections or damage to the pacing wire during handling were also considered.
Electrolyte Imbalances
Post-surgical patients, particularly those in the ICU, often experience electrolyte disturbances. Hypokalemia, hypomagnesemia, or metabolic acidosis can increase the threshold needed for capture, leading to pacing failure.
Myocardial Edema
Myocardial edema secondary to recent surgery and cardiopulmonary bypass can impair the ability of the electrical impulses to propagate through the heart muscle, leading to failure to capture.
Related courses
- Critical Care Nursing Course
- Rhythm interpretation course
- Critical Bytes - Keeping pace with pacing
- ECG interpretation course
References
Image sourced from: Han Naung Tun and Syed Haseeb Raza. “Extreme Bradycardia with Variable Block in Severe Hyperkalemia: A Forgotten Culprit in Brady-Arrhythmia.” Clin Case Rep 10 (2020): 1371

Grace Larson, RN, BN, CertIV(TAE), GradDipClinNurs(PaedCritCare), MAdNursPrac(PaedCritCare), has extensive experience in paediatric nursing, with 13 years in Paediatric Intensive Care Units (PICU). She’s published journal articles in the specialty area of pain and sedation in PICU, and has presented at national and international conferences on the area of pain and sedation in paediatrics. Grace has previously worked with the ACCCN delivering Paediatric Advanced Life Support in Victoria, bringing a wealth of experience into her clinical teaching on paediatric resuscitation. She has also consulted with NSW Health on quality and safety delivering within PICU, and has been contracted with the ANMF to develop nursing programs for nurses who require additional education as part of their practice requirements.
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreFollow James, a 7-year-old boy scheduled for a tonsillectomy and adenoidectomy, as we explore how the 4 P’s of child preparation – Prepare, Play, Parent, Praise – can be used in day surgery to reduce procedural anxiety, support family-centred care, and improve the overall patient experience
Caregiver concern is a powerful predictor of clinical deterioration in children, often surpassing abnormal vital signs. A recent Lancet study confirms its association with ICU admission and ventilation. Integrating caregiver input into assessments, documentation, and escalation protocols can significantly improve early recognition and outcomes in paediatric emergency care.
Medcast Education
Sepsis is a time-critical medical emergency. The National Sepsis Program urges GPs and primary care clinicians to enhance early recognition and management of sepsis to save lives. This update outlines key actions and available resources to support timely diagnosis and intervention across primary care settings.