
Age-related macular degeneration - clinical fact sheet and MCQ
![]()
Overview
Age-related macular degeneration (AMD) is a progressive retinal disease affecting the macula - the central region of the retina responsible for detailed vision. It is the leading cause of severe, irreversible vision loss among individuals over 60 in developed countries, accounting for approximately 8.7% of global blindness. AMD primarily impacts central vision, leading to difficulties in activities such as reading and driving, while peripheral vision remains unaffected.
AMD is broadly classified into:
-
early/intermediate AMD: characterised by the presence of drusen (yellow deposits beneath the retina) and/or pigmentary changes without significant vision loss
-
late AMD, which includes:
-
neovascular (‘wet’) AMD: caused by abnormal blood vessel growth under the macula, leading to leakage and scarring
-
geographic atrophy (‘dry’) AMD: progressive degeneration of retinal pigment epithelial cells, resulting in central vision loss
Diagnosis of age-related macular degeneration
General practitioners should suspect AMD in patients over 50 presenting with:
-
central visual distortion (eg straight lines appearing wavy)
-
difficulty reading or recognising faces
-
reduced central vision
1. Risk factors
Several factors contribute to the development and progression of AMD:
-
age: the most significant risk factor, particularly in individuals over 60
-
family history - having a first degree relative with AMD, quadruples risk. Specific genetic variants, such as Y402H in the CFH gene, increase susceptibility but are not yet used in clinical practice
-
smoking: current smokers have a fourfold increased risk of vision loss due to AMD
-
cardiovascular factors: hypertension and atherosclerosis are associated with a higher risk of late AMD
-
diet: poor dietary habits that lack antioxidants and omega-3 fatty acids may contribute to AMD progression
2. Assessment
-
History: inquire about family history of AMD, smoking status, and cardiovascular health
-
Monocular visual acuity testing: occlude one eye at a time and assess for any reduction in central vision from baseline
-
Fundus examination: look for drusen, pigmentary changes, or signs of neovascularisation, such as retinal haemorrhage
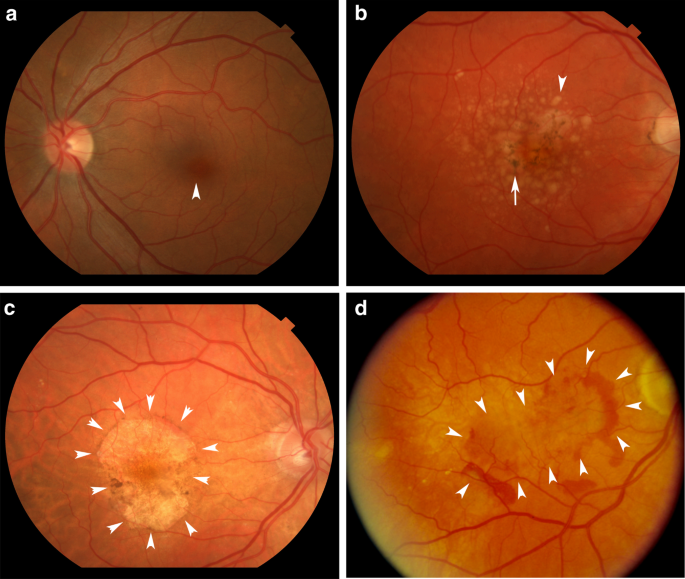
(image credit: Handa et al, 2019) Fundus photographs demonstrating: A) Normal fundus. B) Intermediate AMD with drusen and pigmentary changes. C) Dry AMD with geographic atrophy. D) Neovascular (wet) AMD with subretinal haemorrhage.
-
Amsler grid: use this tool to detect subtle central visual distortions. Patients can be referred to the Macular Disease Foundation page to order a free Amsler grid and for information on how to use it
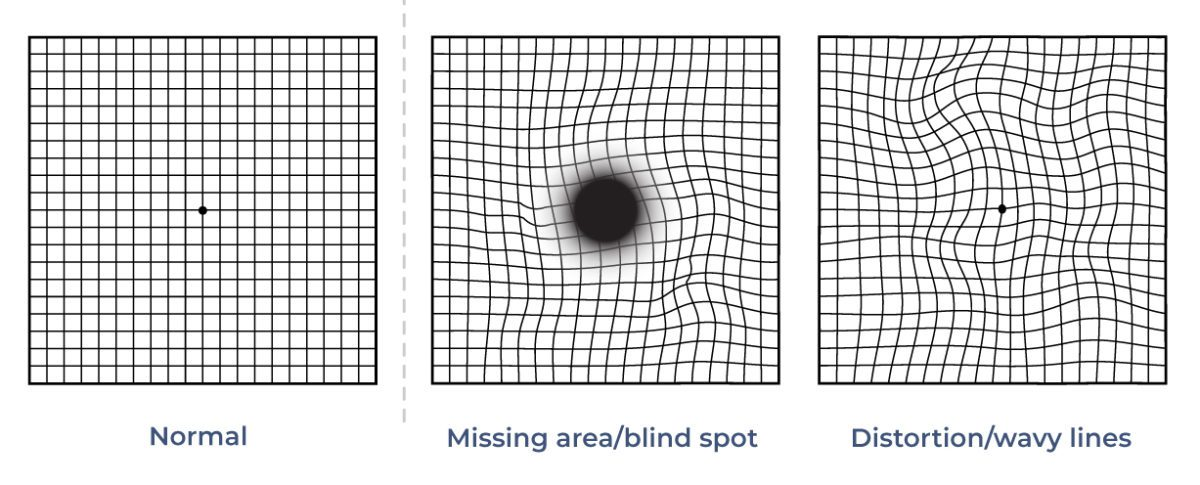
(image credit: https://frontrangeretina.com/how-to-use-an-amsler-grid/)
3. Differential diagnosis
Consider other conditions that can mimic AMD:
-
diabetic macular oedema: associated with diabetes; characterised by retinal haemorrhages and exudates
-
central serous chorioretinopathy (CSR): typically affects younger males; presents with serous retinal detachment
-
macular hole: presents with central vision loss and a full- or partial-thickness foveal defect
-
retinal vein occlusion: sudden unilateral vision loss with retinal haemorrhages and cotton wool spots
-
cataracts: gradual vision loss with lens opacities; does not cause central scotoma
Management of age-related macular degeneration
1. Primary care interventions
-
Lifestyle modifications:
-
smoking cessation: strongly advise patients to quit smoking to reduce AMD progression risk
-
diet: encourage a diet rich in leafy green vegetables, fish, and nuts. Adherence to a Mediterranean diet has been linked to a reduced risk of AMD progression
-
cardiovascular health: manage hypertension and hyperlipidaemia to mitigate associated risks
-
Nutritional supplements: for patients with intermediate AMD in both eyes or advanced AMD in only one eye, consider recommending antioxidant and zinc supplementation as per the Age-Related Eye Disease Study (AREDS) 2 findings
-
Regular monitoring: advise patients to perform regular (eg weekly) self-assessment using the Amsler grid and report any new visual disturbances promptly
-
Education on the importance of regular eye tests
2. Referral criteria
Immediate referral to an ophthalmologist is warranted if:
-
there is sudden onset of central vision loss
-
the patient reports new or worsening visual distortions
-
fundus examination reveals signs of neovascular AMD, such as subretinal haemorrhages or fluid
NOTE: neovascular AMD is a vision-threatening emergency. Early ophthalmological treatment with anti-VEGF therapy can preserve vision.
When referring, include:
-
best corrected visual acuity
-
detailed symptomatology
-
relevant medical and ocular history
-
current medications and any prior ocular treatments
3. Ophthalmological treatments
-
Geographic atrophy: no specific treatment at this stage
-
pegcetacoplan injections (a complement inhibitor) have been TGA-approved, and slow the progression of the atrophic process
-
not routinely used yet as funding is not approved
-
Neovascular AMD: intravitreal injections with anti-vascular endothelial growth factor (anti-VEGF ) maintain vision and prevent severe visual loss
-
this is an ongoing treatment with significant time and cost burden
-
Older treatments such as laser and photodynamic treatment are only rarely used
References
-
Macular Disease Foundation Australia. Everything you need to know about age-related macular degeneration. 2024. (last accessed April 2025).
-
Ruia S, Kaufman EJ. Macular Degeneration. [Updated 2023 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. (last accessed April 2025).
-
Therapeutic Goods Administration. Syfovre – Apellis Australia Pty Ltd [Internet]. Canberra (AU): Australian Government Department of Health and Aged Care. (last accessed April 2025).
-
Royal Victorian Eye and Ear Hospital. Age-related macular degeneration (AMD): primary care management guidelines [Internet]. East Melbourne (AU): Royal Victorian Eye and Ear Hospital; 2022. (last accessed April 2025).
Claim your CPD
After reading the clinical summary above and reviewing the references, complete the quiz to gain 30 minutes of EA CPD and 30 minutes of RP CPD.
You can either self-report CPD to your CPD home, or Medcast will track your learning via your personal CPD Tracker and you can download and report these points once a year. See our CPD Tracker FAQ.
Quiz
Please log in or sign up for a free Medcast account to access the case study questions and achieve the CPD credits.
The Medcast medical education team is a group of highly experienced, practicing GPs, health professionals and medical writers.
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreMedcast Medical Education Team
Many GPs may not see veterans frequently. This FastTrack provides a summary of key steps that can make veteran care efficient, rewarding and well-integrated into routine practice, including links to additional resources. 30mins each of RP and EA are available.
Medcast Medical Education Team
From the 1st Nov 2025, updates to the MBS affect all GPs providing services related to long-acting reversible contraceptives. This FastTrack will get you up to date on which items attracted an increased rebate, the new item number, and how to avoid common compliance pitfalls. 30mins each of RP and EA CPD available with the quiz.
Medcast Medical Education Team
GPs are often faced with the presentation of a red, sticky eye. Even without a slit lamp, there are key points in your clinical assessment that can help to differentiate the causes of conjunctivitis and guide the appropriate management. Read the fact sheet then claim 30mins each of RP and EA CPD with the quiz.